Demystifying the side effects of cancer therapy
One common perception is that, while undergoing treatment for cancer, the patient will undergo terrible and unbearable side effects. While it would be rare to have patients go through their treatment with zero side effects, the truth is that modern medicine has come a long way in reducing them, such that most patients can complete their treatment courses fairly smoothly. With the correct knowledge, patients can also help themselves through daily lifestyle measures that complement their doctor’s management of these side effects.
Part One: Radiotherapy
When a patient receives radiation therapy he or she does not feel any pain, heat or cold from it. Side effects can occur as some healthy tissues near the treatment area can get damaged by the radiation. Side effects are divided into early and late. Early side effects occur during radiation and go away a few weeks after. Late side effects occur months to years after the radiation therapy, and may be permanent. How bad these long-term side effects are depend a lot on how much radiation dose each surrounding organ receives. As radiotherapy technology (see below) advances, radiation oncologists have been able to more precisely target tumour tissue and avoid healthy tissue, resulting in fewer side effects.
3D-CRT
IMRT
SBRT
SRS
Proton Therapy
Individual Side Effects
Fatigue
Radiotherapy can produce fatigue, or tiredness, that tends to be less severe and does not last as long as after chemotherapy. Upon completion, energy levels start to improve gradually. Those who are anxious, or depressed prior to radiotherapy tend to experience greater levels of fatigue after radiotherapy.
What the doctor can do to minimise fatigue
Advances in precision of radiation therapy techniques can reduce fatigue. Fatigue is related to the amount of healthy tissue being radiated. A patient receiving radiation to the whole brain for spread of cancer to the brain can experience severe fatigue. Stereotactic radiosurgery, or the precise, high dose targeting of individual brain tumours, significantly reduces the rate of fatigue because much more normal brain tissue is spared from radiation.

Dose distribution difference between WBRT (left) and SRS (right). A typical dose distribution on a planning-CT of WBRT on the left side and SRS on the right side. With WBRT, the healthy brain tissue receives the same low palliative radiation dose (non-ablative). With SRS, only the metastatic tissue receives a high ablative dose. (Reference: BioMed Central, 2017)
What the patient can do
Xerostomia (Dry mouth)
Xerostomia or dry mouth is common during and after radiotherapy to the head and neck area, due
to exposure of the salivary glands to radiotherapy. Saliva flow of affected glands is reduced by half in the first week of radiotherapy, then gradually declines as treatment continues. Despite this, there can be some recovery as the patient gets used to the sensation and as the other salivary glands compensate by producing more saliva.
Dry mouth should be managed as it can lead to other problems like affecting swallowing, loss of
appetite, sleep disruption and poor dental hygiene.
What the doctor does to reduce and treat xerostomia
Use of highly conformal radiation therapy techniques like intensity modulated radiotherapy (IMRT) help to avoid more of the salivary glands without affecting treatment of the tumour. A clinical trial has demonstrated that use of IMRT in head and neck cancers reduces dry mouth and leads to faster recovery of saliva flow, with associated improvements in quality of life.
Medications like pilocarpine have been shown to increase saliva flow and may be prescribed by the radiation oncologist if necessary.
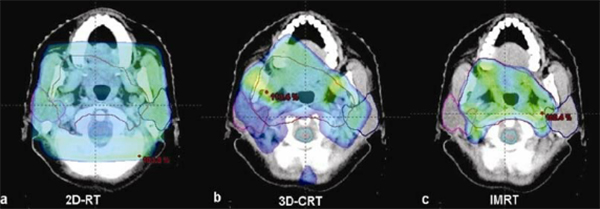
Fig. 1 Axial planning CT slice showing typical dose-wash of (a) conventional radiotherapy (2D-RT); (b) 3D-CRT; and (c) IMRT plan for head-neck cancer. Note the progressive high-dose conformation to the target volume and sparing of surrounding normal structures (Indian J Surg Oncol, 2010)
What the patient can do
Oral mucositis
Radiation therapy to the head and neck can injure the lining, or mucosa, of the mouth. This can lead to painful mouth ulcers that can affect one’s ability to eat and drink. Thankfully, there are measures that can be taken by both patient and doctor to manage this.
What the doctor does to reduce and manage oral mucositis
Just like in the case of xerostomia, expert use of IMRT can minimise dose to the oral mucosa that is not at risk of harbouring cancer cells and thereby reduce the severity of the mucositis.
The radiation oncologist will also prescribe anti-inflammatory lozenges and rinses like difflam that help reduce the number and severity of painful mouth ulcers. To treat painful mucositis,
combination mouthwashes with local anaesthetic effect provide comfort. If necessary, painkillers will be given and adjusted as necessary.
What the patient can do
Gastrointestinal mucositis
The lining of the gastrointestinal tract from oesophagus to the rectum can similarly be affected by radiotherapy. What the patient experiences from this depends on the area treated.
When the abdomen is treated, patients may get nausea and occasionally vomiting. In those patients, who are at a higher risk from this, the doctor will prescribe an anti-nausea/vomiting tablet like ondansetron prior to radiotherapy as prevention. Patients may also find that drinking peppermint or ginger tea is helpful with this.
When the abdomen or pelvis is treated, diarrhoea can occur and in the first instance can be reduced by taking an anti-diarrhoeal like loperamide, which slows down the intestines. There is increasing evidence that taking probiotics daily throughout the course of radiation also reduces the incidence of diarrhoea. Probiotics are live bacteria or yeasts that help restore the balance of ‘good’ and ‘bad’ bacteria in the intestines, protecting the intestinal lining from injury. When you have diarrhoea, ensure hydration levels by taking 2.5-3 litres of water per day.
Examples of how advanced technologies reduce gastrointestinal side effects
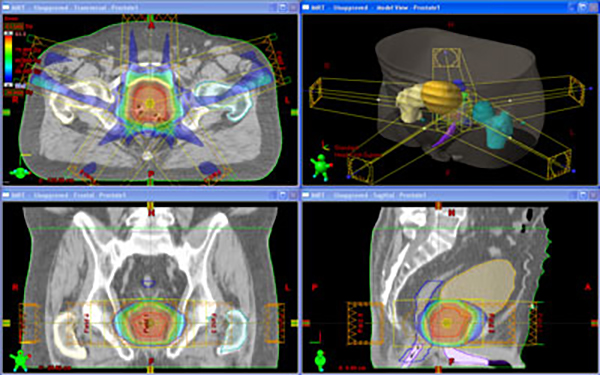
The use of IMRT allows the radiation oncologist to curve the radiation doses to avoid the intestines and therefore reduce the incidence of diarrhoea. This technique can be employed in many tumour types to reduce mucositis including pancreatic, gynaecological and prostate cancers.

Comparative dose distributions for A)) 4FLD, and B) IMRT. (Cureus, 2016)
In the case of prostate cancers, the rectum is located just behind the prostate and cannot be
completely avoided during radiotherapy. Yet high doses of radiation are required to destroy prostate cancers. Advanced radiation techniques achieve this in a couple of ways. Firstly, IMRT is used which allows the high dose radiation area to be curved to follow the shape of the prostate, so that just a small sliver of rectum is in this area. Secondly, using scanning technology available at the treatment unit itself, the prostate is seen directly and treatment area adjusted daily to ensure full target coverage. This daily image-guidance allows the radiation oncologist to reduce the safety margins needed to cover the prostate and therefore minimize injury to the rectum.
Radiation Dermatitis
Radiation beams must enter and exit through the surface of the body to reach the tumour. Radiation injury to the skin can therefore occur. In the past, radiation beams were of lower penetrating power and therefore skin doses were high and resulted in many patients having bad skin burns. However, modern radiation therapy beams have a skin sparing effect, which can be further fine-tuned with IMRT. Therefore, skin reactions, while inevitable, are overall less severe than before, unless the tumour is close to the skin. Radiotherapy to the whole brain can also result in complete scalp hair loss which takes 3-6 months to grow back.
After starting radiotherapy, mild skin redness is seen as early as after 10-14 hours in the area being treated. In the weeks after, the skin gradually gets dryer and redder, may become itchy, and the hair in that area may fall – all very tolerable changes. In some cases, after 4-5 weeks the skin may breakdown and become weepy. The severity peaks at 1-2 weeks after radiotherapy, then starts to improve, with complete healing in 1-3 months.
How the radiation oncologist can use advanced technologies to reduce radiation dermatitis
Patient undergoing whole brain radiotherapy typically lose all their scalp hair temporarily, due to the x-rays passing through the scalp hair follicles to reach the brain. With advanced delivery methods like volumetric arc therapy (VMAT) or Tomotherapy, the radiation oncologist is able to spread out the dose to the scalp as the x-ray beams come from almost 360 degrees. This spread out dose is lower than that received by the scalp without compromising coverage of the brain. The result is potentially less scalp dermatitis and much reduced hair loss
What you can do to minimize and manage radiation dermatitis
How the radiotherapy team manages radiation dermatitis
If the skin is itchy, your radiation oncologist may prescribe steroid creams to relieve it. When there is skin breakdown, the key is to keep the area clean and free of infection. The wound will need to be assessed by the nurse and dressed with non-stick gel or foam dressings. If there is infection, dressings containing silver, which has antimicrobial action, are used.
Radiation Cystitis
Radiotherapy to pelvic organs like the prostate, cervix, uterus and bladder can give rise to inflammation of the bladder, or cystitis. The patient may need to pass urine more often and experience more urge as well as a stinging sensation during urination.
What you can do
What the doctor can do
If these measures do not provide enough relief, the radiation oncologist will prescribe medications that can reduce urinary irritation, frequency and improve urine flow.
How we support you at AARO
At AARO, our top concern is the safe and precise delivery of radiation treatment for all our patients. Utilizing top-of- the-line radiotherapy techniques and systems, our experienced doctors meticulously plan each step of your treatment so that only the tumor and at-risk areas are treated with maximal normal tissue sparing. Our friendly and attentive Senior Radiation Therapists will also be on hand throughout the duration of your radiotherapy to render advice and direct you to the doctors should there be a need. Here are some steps AARO has set in place to ensure prompt diagnosis and treatment of any radiation side effects:
1) At least weekly review by AARO doctors during the course of your treatment
2) Telephone hotline to our Senior Radiation Therpists accessible anytime during office hours
for any concerns you may face (65) 8101 3838, available on Whatsapp, Viber and WeChat.
3) AARO has also put together our own in-house Radiotherapy Side Effect Packages consisting of essential medications, creams and supportive items, together with information on the lifestyle “tips and tricks” to help you through radiotherapy.
These packages are specific to your tumor site and are available upon request or as part of your consultation.


